Der Vagusnerv: Die verborgene Brücke zwischen Körper und Geist
The vagus nerve is often reduced to a wellness talking point. In reality, it is a bidirectional regulatory system integrating brainstem function, interception, autonomic balance, immune signalling, and organ regulation. Approximately 80% of its fibres are afferent, carrying information from the body to the brain. This reframes the hierarchy: The brain is not leading regulation.
It is responding to the body’s state. What we call “emotional experience” is, in large part, interpreted through interoceptive signalling. If those signals are distorted, inconsistent, or biased toward threat, cognition reorganizes around that physiology—not the other way around.
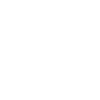
First, let's dive into the anatomy of this extraordinary nerve. Watch this great video tutorial
Regulation Is a Brainstem Function Before It Is Psychological
Clinical work repeatedly confirms a simple reality: Cognitive insight does not reorganize the autonomic state. A patient can have full narrative awareness and remain physiologically locked in sympathetic activation or dorsal vagal shutdown. This is because regulation is mediated primarily through subcortical structures:
- Nucleus tractus solitarius (NTS)
- Dorsal motor nucleus of the vagus
- Nucleus ambiguus
- Reticular formation
These systems operate below conscious control and determine:
- Heart rate variability
- Respiratory rhythm
- Digestive function
- Vocal tone and social engagement capacity
Without shifts at this level, cortical intervention has limited reach
The Clinical Problem: Misinterpreted Safety
In dysregulated systems, the issue is rarely “too much stress.”It is miscalibrated neuroception. The system detects threats where there are none, or fails to register safety when it is present. This is not a psychological distortion. It is a bottom-up error in sensory integration and prediction. The result:
- Persistent sympathetic bias (hypervigilance, inflammation, tension)
- Dorsal collapse (fatigue, dissociation, low-tone states)
- Reduced vagal flexibility (poor state transitions)
This is why many patients plateau despite doing everything “correctly.”The system is not lacking tools.
It is lacking accurate input.
Why Technique-Driven Models Plateau
More interventions do not equal more regulation. In fact, excessive input into an unstable system often amplifies dysregulation. Protocols assume capacity.
But capacity is the very function that is compromised. If vagal tone is low and interoceptive accuracy is poor, the system cannot:
- Differentiate signal from noise
- Integrate new input
- Stabilize after activation
This leads to cycles of temporary relief followed by regression. This is not clinical failure. It is predictable physiology.
Manual Therapy as a Regulatory Interface
Body-based work is not adjunctive—it is a primary access point. Touch interfaces directly with:
- C-tactile afferents (linked to insular processing and affect regulation)
- Mechanoreceptors influencing vagal pathways
- Fascial and interoceptive networks feeding into the NTS
When applied with precision, it provides structured, non-threatening sensory input that recalibrates prediction models in the nervous system.Not through force.Through timing, accuracy, and coherence.
Shiatsu as a Vagal Modulation System
At a high level, Shiatsu is not simply pressure along meridians. It is a regulatory dialogue with the autonomic nervous system. The key variables are not just location, but:
- Rhythm
- Depth
- Continuity
- Relational presence
- Practitioner state
These variables influence vagal pathways through:
- Respiratory entrainment
- Cardiac variability shifts
- Modulation of muscle tone and fascial tension
Reorganization begins when the system experiences:
- Predictable, coherent input
- Non-threatening contact
- Gradual shifts without overwhelm
Neuroception is recalibrated experientially—not cognitively.
Clinically, I have seen Shiatsu restore regulation in individuals where talk therapy, medication, or exercise alone failed. This is because Shiatsu does not ask the nervous system to understand safety — it allows the body to experience it. Shiatsu meets the nervous system where trauma actually lives: in tone, breath, tissue, and rhythm.

From Intervention to Reorganization
Effective work at this level does not “fix symptoms.”It alters the conditions that generate them. As vagal regulation improves:
- Heart rate variability increases
- Inflammatory signalling decreases
- Digestive function normalizes
- Affective stability improves
Symptoms resolve as a downstream effect of system reorganization. Not as isolated targets.
Clinical Implication
If the nervous system cannot accurately detect safety, it cannot sustain healing. No protocol overrides that.The work is not adding more. It is refining input until the system updates its internal model of the world. From doing more to the system
→ to give the system what it can actually use
Clinical Case Study 1: Chronic Sympathetic Activation
A 42-year-old practitioner presented with long-standing neck and shoulder tension, shallow breathing, digestive irregularity, and persistent low-grade anxiety. She had already done extensive work—therapy, breathwork, somatic practices—and had strong cognitive awareness of her patterns. Despite this, her baseline state remained activated.
Assessment revealed:
- Elevated resting muscle tone through the cervical and thoracic regions
- Limited diaphragmatic movement
- Irregular breath rhythm with shortened exhale
- Low heart rate variability patterns (inferred clinically through breath and pulse quality)
- High interoceptive vigilance, but low accuracy (misinterpreting neutral sensations as threat)
The intervention did not focus on releasing tension directly.Instead, sessions emphasized:
- Slow, predictable pressure with extended contact time
- Work through the abdomen and ribcage to influence respiratory rhythm
- Minimal variation in input to reduce sensory load
- Practitioner-regulated pacing to entrain a slower autonomic rhythm
Within three sessions, measurable shifts began to emerge:
- Spontaneous lengthening of the exhale
- Visible reduction in accessory breathing patterns
- Softening of cervical tone without direct mechanical release
- Improved digestive regularity
More importantly, the patient reported a new internal reference point:
“I can feel what calm actually is in my body, not just in my mind.”This marked the transition from effort-based regulation to state-based regulation. The symptoms did not need to be chased further. They began resolving as the system stabilized.
Clinical Case Study 2: Dorsal Vagal Collapse and Fatigue
A 55-year-old male presented with chronic fatigue, low motivation, digestive slowdown, and intermittent dissociation. Medical testing was largely unremarkable. He had been treated primarily through supplementation and lifestyle interventions with limited change. Clinical presentation suggested dominant dorsal vagal patterning:
- Low vocal tone and reduced facial expressivity
- Slowed responses and low affect variability
- Cold extremities
- Collapsed postural patterns
- Shallow, irregular breathing with frequent pauses
The key clinical error in cases like this is attempting to “energize” the system too quickly. Instead, the work focused on graded activation within a regulated window:
- Gentle, rhythmic contact rather than deep pressure
- Emphasis on continuity of touch to maintain safety
- Subtle mobilization of the thoracic region to support breath without forcing it
- Tracking micro-responses to avoid pushing into further shutdown
Over the course of several sessions:
- Breathing became more continuous and less interrupted
- Skin tone and peripheral warmth improved
- Eye contact increased spontaneously
- Speech gained variation in tone and pace
By session five, the patient reported:
“I don’t feel like I’m pushing myself to function anymore. There’s more natural energy.”
This is a critical distinction. The goal was not stimulation, but restoration of the autonomic range. As ventral vagal function began to re-emerge, energy was no longer forced—it became available.

The vagus nerve is not a technique or a trend. It is a central regulator of how experience is constructed. When it is dysregulated, patients live in adaptive survival physiology. When flexibility returns, the system regains range.
With range comes:
- Choice
- Recovery
- Responsiveness
That is where meaningful clinical change begins.

Shiatsu Therapy and NeuroPath Reset Method are not add-ons to healing — they are expressions of a deeper truth: Healing happens when the nervous system remembers how to feel safe in the body.
The vagus nerve is the biological doorway. Touch, presence, rhythm, and attuned guidance are the keys. When we stop trying to fix the body and instead restore its regulatory intelligence, symptoms lose their purpose. And what remains is resilience, connection, and choice.
The vagus nerve is not a trend. It is not a hack. It is the biological foundation of embodiment, presence, and resilience. When we restore vagal integrity, we restore choice. And choice is the opposite of trauma.
Sincerely yours,
Mihael Mamychshvili
Founder, NeuroPath Reset Method
*For in-person trainings, go to:https://www.neuropathresetmethod.com/workshops-retreats
*For online courses: https://www.neuropathresetmethod.com/online-courses